国际生殖健康/计划生育杂志 ›› 2026, Vol. 45 ›› Issue (3): 209-213.doi: 10.12280/gjszjk.20250562
谢晓冰, 侯涛( )
)
XIE Xiao-bing, HOU Tao()
摘要:
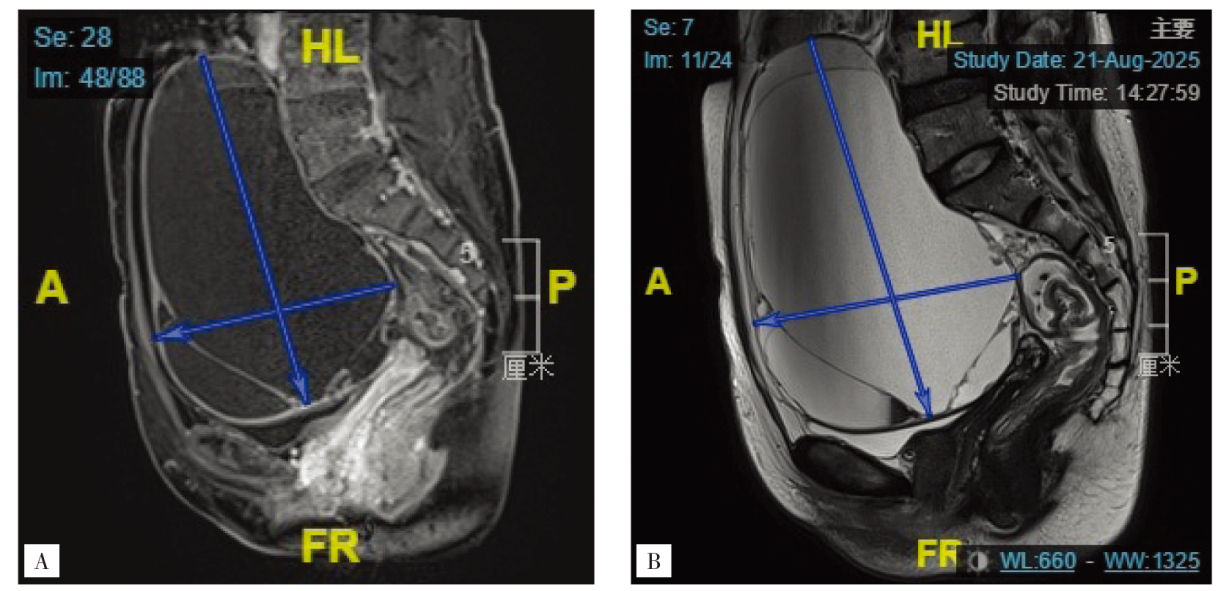
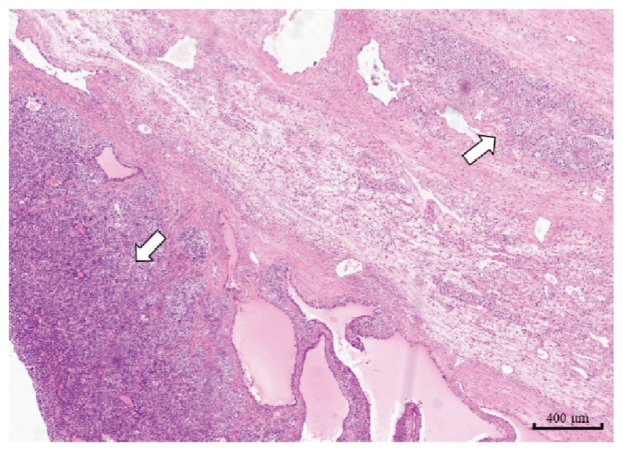
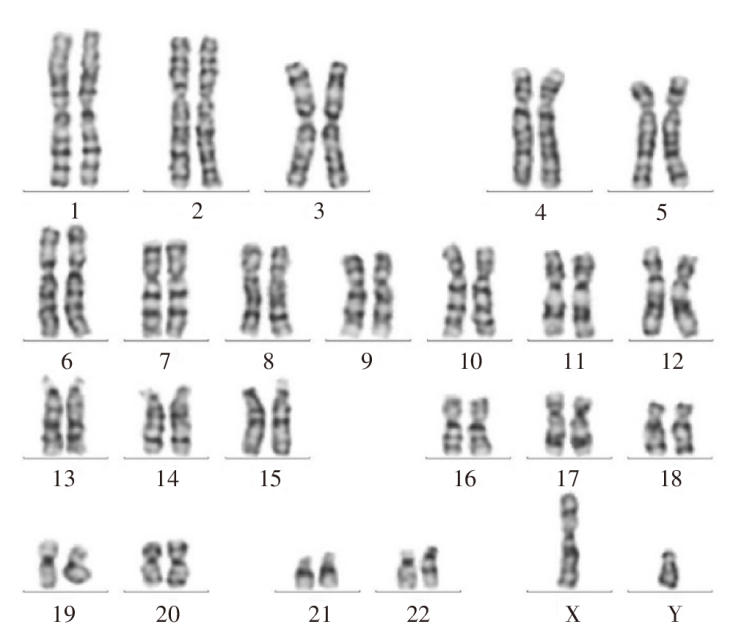
完全型雄激素不敏感综合征(complete androgen insensitivity syndrome,CAIS)是一种X连锁隐性遗传病,由雄激素受体基因突变导致,临床较为罕见,且合并两性母细胞瘤的相关病例更为鲜有。报告1例染色体核型为46,XY,社会性别为女性,且合并双侧卵巢两性母细胞瘤的病例。患者为53岁原发性闭经女性,因下腹隐痛就诊,查体女性第二性征及外阴发育正常,术前雌二醇与抑制素B水平升高,影像学检查提示盆腔巨大包块(直径约16 cm)、子宫显示不清。术中见左侧卵巢肿瘤,右侧附件外观正常,右侧附件连接一肌性组织,大小约4 cm×2 cm,考虑始基子宫。遂行左侧附件切除术,术中冰冻病理提示交界性或低度恶性肿瘤,进一步行全面分期手术,术后病理最终诊断两性母细胞瘤。术后外周血染色体核型分析示46,XY。此类患者需做到早期诊断与干预,从根本上预防其性腺肿瘤的发生。