国际生殖健康/计划生育 ›› 2022, Vol. 41 ›› Issue (5): 353-359.doi: 10.12280/gjszjk.20220299
• 论著 • 下一篇
沈鉴东, 谢佳孜, 吴畏, 蔡令波, 汪道武, 刘嘉茵, 刁飞扬( )
)
收稿日期:2022-06-15
出版日期:2022-09-15
发布日期:2022-10-12
通讯作者:
刁飞扬
E-mail:phenix_y@163.com
基金资助:
SHEN Jian-dong, XIE Jia-zi, WU Wei, CAI Ling-bo, WANG Dao-wu, LIU Jia-yin, DIAO Fei-yang()
Received:2022-06-15
Published:2022-09-15
Online:2022-10-12
Contact:
DIAO Fei-yang
E-mail:phenix_y@163.com
摘要:
目的:分析伴有性染色体异常不孕夫妇行植入前遗传学检测(preimplantation genetic testing,PGT)的结局,探讨夫妻双方之一性染色体异常导致胚胎性染色体异常的风险,以及PGT在相关人群中的应用价值。方法:回顾性分析南京医科大学第一附属医院生殖医学科伴有性染色体异常同时行PGT治疗的夫妇的胚胎染色体检测结果以及胚胎移植结局。PGT策略采用囊胚期活检,活检材料经过全基因组扩增后,采用全基因组低深度测序分析染色体拷贝数改变。在复苏周期中,统计可移植胚胎移植后的临床妊娠结局。结果:在性染色体异常的23对夫妇(其中包括47,XYY及其嵌合体6例、47,XXY及其嵌合体2例、47,XXX 4例、45,X嵌合体8例、女性X染色体节段性缺失3例)的24个促排卵周期中,共获得可检测囊胚77枚,明确诊断76枚(98.70%),其中40枚(52.63%)为整倍体可移植胚胎,13枚(17.10%)非整倍体嵌合体胚胎,23枚(30.26%)为非整倍体不可移植胚胎。在3例X染色体节段性缺失患者中所有异常胚胎均为X染色体节段性缺失,而其他性染色体数目异常患者中共发现3枚(3.95%)性染色体嵌合体非整倍体胚胎。在18个复苏移植周期中,共获得9例(50.00%)健康活产。结论:性染色体数目非整倍体异常夫妇的胚胎性染色体异常风险较低,在辅助生殖技术助孕过程中PGT并不是必需的治疗方案;而性染色体节段性非整倍体夫妇胚胎性染色体异常风险较高,结合卵巢功能情况以及在患者充分知情同意的情况下,可酌情考虑PGT,降低后代性染色体异常风险。
沈鉴东, 谢佳孜, 吴畏, 蔡令波, 汪道武, 刘嘉茵, 刁飞扬. 胚胎植入前遗传学检测在性染色体异常夫妇助孕中的应用[J]. 国际生殖健康/计划生育, 2022, 41(5): 353-359.
SHEN Jian-dong, XIE Jia-zi, WU Wei, CAI Ling-bo, WANG Dao-wu, LIU Jia-yin, DIAO Fei-yang. Application of Preimplantation Genetic Testing in Assisted Reproductive Therapy for Couples with Sex Chromosome Abnormalities[J]. Journal of International Reproductive Health/Family Planning, 2022, 41(5): 353-359.
| 活检周期序号 | 女方年龄(岁) | 男方年龄(岁) | 女方bFSH(IU/L) | 女方窦卵泡计数(个) | 女方AMH(ng/mL) | 男方/女方染色体核型 |
|---|---|---|---|---|---|---|
| 1 | 30 | 28 | 6.68 | 20 | / | 47,XYY |
| 2 | 26 | 30 | 8.86 | 12 | 4.31 | 47,XYY |
| 3 | 31 | 28 | 6.92 | 19 | 8.95 | 47,XYY |
| 4 | 21 | 26 | 10.22 | 20 | 1.93 | 47,XYY |
| 5 | 28 | 32 | 5.89 | 14 | 3.90 | 47,XYY |
| 6 | 23 | 25 | 7.38 | 8 | 1.96 | 47,XYY[65]/45,X[35] |
| 7 | 27 | 32 | 5.28 | 20 | 6.60 | 47,XXY |
| 8 | 28 | 29 | 10.93 | 11 | 0.75 | 47,XXY[77]/46,XY[23] |
| 9 | 26 | 27 | 12.70 | 3 | 0.36 | 47,XXX |
| 10 | 25 | 25 | 6.02 | 20 | 7.34 | 47,XXX |
| 11 | 27 | 28 | 4.85 | 14 | 7.62 | 47,XXX |
| 12 | 29 | 48 | 6.16 | 7 | 1.10 | 47,XXX |
| 13 | 28 | 26 | 5.47 | 12 | 7.71 | 45,X[95]/47,XXX[5] |
| 14 | 30 | 30 | 8.60 | 15 | 6.86 | 45,X[4]/46,XX[46] |
| 15 | 41 | 33 | 5.98 | 6 | 2.53 | 45,X[?]/46,XX[?] |
| 16* | 36 | 34 | 8.89 | 5 | 1.89 | 45,X[5]/46,XX[45] |
| 17* | 37 | 35 | 8.89 | 5 | 1.89 | 45,X[5]/46,XX[45] |
| 18 | 31 | 30 | / | 18 | 8.13 | 45,X,15ps+[4]/46,XX,15ps+[114] |
| 19 | 35 | 39 | 7.20 | 15 | 5.35 | 45,X[5]/46,XX[95] |
| 20 | 32 | 31 | 14.18 | 3 | 0.23 | 45,X[35]/46,X,del(p21) |
| 21 | 33 | 37 | 7.07 | 6 | 2.60 | 45,X[49]/47,XXX[51] |
| 22 | 28 | 27 | 4.88 | 11 | 4.40 | 46,X,der(X)t(X;Y)(p22.3;q11.2) |
| 23 | 25 | 23 | 6.60 | 8 | 1.13 | 46,X,del(X)(p21) |
| 24 | 26 | 29 | 15.58 | 6 | 0.20 | 46,X,del(X)(q22.3q27.1) |
表1 活检周期患者年龄及女方卵巢功能
| 活检周期序号 | 女方年龄(岁) | 男方年龄(岁) | 女方bFSH(IU/L) | 女方窦卵泡计数(个) | 女方AMH(ng/mL) | 男方/女方染色体核型 |
|---|---|---|---|---|---|---|
| 1 | 30 | 28 | 6.68 | 20 | / | 47,XYY |
| 2 | 26 | 30 | 8.86 | 12 | 4.31 | 47,XYY |
| 3 | 31 | 28 | 6.92 | 19 | 8.95 | 47,XYY |
| 4 | 21 | 26 | 10.22 | 20 | 1.93 | 47,XYY |
| 5 | 28 | 32 | 5.89 | 14 | 3.90 | 47,XYY |
| 6 | 23 | 25 | 7.38 | 8 | 1.96 | 47,XYY[65]/45,X[35] |
| 7 | 27 | 32 | 5.28 | 20 | 6.60 | 47,XXY |
| 8 | 28 | 29 | 10.93 | 11 | 0.75 | 47,XXY[77]/46,XY[23] |
| 9 | 26 | 27 | 12.70 | 3 | 0.36 | 47,XXX |
| 10 | 25 | 25 | 6.02 | 20 | 7.34 | 47,XXX |
| 11 | 27 | 28 | 4.85 | 14 | 7.62 | 47,XXX |
| 12 | 29 | 48 | 6.16 | 7 | 1.10 | 47,XXX |
| 13 | 28 | 26 | 5.47 | 12 | 7.71 | 45,X[95]/47,XXX[5] |
| 14 | 30 | 30 | 8.60 | 15 | 6.86 | 45,X[4]/46,XX[46] |
| 15 | 41 | 33 | 5.98 | 6 | 2.53 | 45,X[?]/46,XX[?] |
| 16* | 36 | 34 | 8.89 | 5 | 1.89 | 45,X[5]/46,XX[45] |
| 17* | 37 | 35 | 8.89 | 5 | 1.89 | 45,X[5]/46,XX[45] |
| 18 | 31 | 30 | / | 18 | 8.13 | 45,X,15ps+[4]/46,XX,15ps+[114] |
| 19 | 35 | 39 | 7.20 | 15 | 5.35 | 45,X[5]/46,XX[95] |
| 20 | 32 | 31 | 14.18 | 3 | 0.23 | 45,X[35]/46,X,del(p21) |
| 21 | 33 | 37 | 7.07 | 6 | 2.60 | 45,X[49]/47,XXX[51] |
| 22 | 28 | 27 | 4.88 | 11 | 4.40 | 46,X,der(X)t(X;Y)(p22.3;q11.2) |
| 23 | 25 | 23 | 6.60 | 8 | 1.13 | 46,X,del(X)(p21) |
| 24 | 26 | 29 | 15.58 | 6 | 0.20 | 46,X,del(X)(q22.3q27.1) |
| 活检周期 序号 | 男方/女方染色体核型 | 活检 囊胚数 | 确诊 囊胚数 | 整倍体 胚胎数 | 嵌合体 胚胎结果 | 非整倍体异常 胚胎结果 | 复苏周期 移植结局 |
|---|---|---|---|---|---|---|---|
| 1 | 47,XYY | 7 | 7 | 5 | / | +7; +5 | 活产 |
| 2 | 47,XYY | 1 | 1 | 1 | / | / | 活产 |
| 3 | 47,XYY | 3 | 3 | 2 | / | -18 | 未孕 |
| 4 | 47,XYY | 1 | 1 | 1 | / | / | 活产 |
| 5 | 47,XYY | 5 | 5 | 3 | -1(q31.3-qter)(mos, 23%) | +7(q11.23-qter) | / |
| 6 | 47,XYY[65]/45,X[35] | 3 | 3 | 1 | / | +1(q32.1-qter); -22 | 活产 |
| 小计 | 20 | 20 | 13 | 1 | 6 | ||
| 7 | 47,XXY | 3 | 3 | 2 | / | +4(q28.3-qter) | 自然流产 |
| 8 | 47,XXY[77]/46,XY[23] | 2 | 2 | 1 | -22(mos, 22%) | / | 未孕 |
| 小计 | 5 | 5 | 3 | 1 | 1 | ||
| 9 | 47,XXX | 1 | 1 | 1 | / | / | 活产 |
| 10 | 47,XXX | 8 | 8 | 3 | +14(mos, 22%), +15(mos, 23%), -18(mos,29%), +X(mos, 34%); +1(mos, 28%),-3(mos, 39%),-7(mso, 32%),+9(mos, 32%),+15(mos, 24%),-18(mos, 28%),+Y(mos, 23%); +15(mos, 36%) | -1(p31.1-pter); -7(q21.11-qter) | 活产 |
| 11 | 47,XXX | 3 | 3 | 3 | / | / | / |
| 12 | 47,XXX | 2 | 2 | 2 | / | / | 未孕;活产 |
| 小计 | 14 | 14 | 9 | 3 | 2 | ||
| 13 | 45,X[95]/47,XXX[5] | 3 | 3 | 1 | -14(mos, 30%) | +2(mos,45%),-21 | / |
| 14 | 45,X[4]/46,XX[46] | 5 | 4 | 2 | +9p(mos, 42%), -9q(mos, 59%), -18(mos, 34%) | -16 | 未孕 |
| 15 | 45,X[?]/46,XX[?] | 1 | 1 | 1 | / | / | 未孕 |
| 16* | 45,X[5]/46,XX[45] | 1 | 1 | 1 | / | / | /# |
| 17* | 45,X[5]/46,XX[45] | 5 | 5 | 3 | / | -7(p22.1-pter);+17 | 未孕 |
| 18 | 45,X,15ps+[4]/46,XX,15ps+[114] | 4 | 4 | 1 | / | +19;-12(q24.31-qter);-16 | 活产 |
| 19 | 45,X[5]/46,XX[95] | 6 | 6 | 0 | +5(mos, 26%), -19(mos, 21%); -3(q11.2-qter)(mos, 32%), -16(mos, 26%), -18(p11.21-pter)(mos, 41%), +4(q13.1-qter)(mos, 25%), +7(q31.33-qter)(mos, 37%), +11(q14.3-qter)(mos, 34%), +13(q31.3-qter)(mos, 36%), +14(q22.3-qter)(mos, 51%); -1(mos, 23%), -16(mos,26%) | +21,-X(q25-qter)(mos, 42%); Triploid; Triploid | 自然流产 |
| 20 | 45,X[35]/46,X,del(p21) | 1 | 1 | 0 | -2(q14.1-qter)(mos, 29%) | / | 自然流产 |
| 21 | 45,X[49]/47,XXX[51] | 6 | 6 | 4 | +15(mos, 26%), +22(mos, 25%) | -18 | / |
| 小计 | 32 | 31 | 13 | 7 | 11 | ||
| 22 | 46,X,der(X)t(X;Y)(p22.3;q11.2) | 3 | 3 | 2 | / | -X(p22.31-pter), +Y(q11.221-qter) | / |
| 23 | 46,X,del(X)(p21) | 2 | 2 | 0 | +3(mos, 26%) | -X(p21.3-pter) | 活产 |
| 24 | 46,X,del(X)(q22.3q27.1) | 1 | 1 | 0 | / | -X(q22.3-q27.1) | / |
| 小计 | 6 | 6 | 2 | 1 | 3 | ||
| 总计 | 77 | 76 | 40 | 13 | 23 |
表2 活检周期胚胎检测结果及复苏移植结局
| 活检周期 序号 | 男方/女方染色体核型 | 活检 囊胚数 | 确诊 囊胚数 | 整倍体 胚胎数 | 嵌合体 胚胎结果 | 非整倍体异常 胚胎结果 | 复苏周期 移植结局 |
|---|---|---|---|---|---|---|---|
| 1 | 47,XYY | 7 | 7 | 5 | / | +7; +5 | 活产 |
| 2 | 47,XYY | 1 | 1 | 1 | / | / | 活产 |
| 3 | 47,XYY | 3 | 3 | 2 | / | -18 | 未孕 |
| 4 | 47,XYY | 1 | 1 | 1 | / | / | 活产 |
| 5 | 47,XYY | 5 | 5 | 3 | -1(q31.3-qter)(mos, 23%) | +7(q11.23-qter) | / |
| 6 | 47,XYY[65]/45,X[35] | 3 | 3 | 1 | / | +1(q32.1-qter); -22 | 活产 |
| 小计 | 20 | 20 | 13 | 1 | 6 | ||
| 7 | 47,XXY | 3 | 3 | 2 | / | +4(q28.3-qter) | 自然流产 |
| 8 | 47,XXY[77]/46,XY[23] | 2 | 2 | 1 | -22(mos, 22%) | / | 未孕 |
| 小计 | 5 | 5 | 3 | 1 | 1 | ||
| 9 | 47,XXX | 1 | 1 | 1 | / | / | 活产 |
| 10 | 47,XXX | 8 | 8 | 3 | +14(mos, 22%), +15(mos, 23%), -18(mos,29%), +X(mos, 34%); +1(mos, 28%),-3(mos, 39%),-7(mso, 32%),+9(mos, 32%),+15(mos, 24%),-18(mos, 28%),+Y(mos, 23%); +15(mos, 36%) | -1(p31.1-pter); -7(q21.11-qter) | 活产 |
| 11 | 47,XXX | 3 | 3 | 3 | / | / | / |
| 12 | 47,XXX | 2 | 2 | 2 | / | / | 未孕;活产 |
| 小计 | 14 | 14 | 9 | 3 | 2 | ||
| 13 | 45,X[95]/47,XXX[5] | 3 | 3 | 1 | -14(mos, 30%) | +2(mos,45%),-21 | / |
| 14 | 45,X[4]/46,XX[46] | 5 | 4 | 2 | +9p(mos, 42%), -9q(mos, 59%), -18(mos, 34%) | -16 | 未孕 |
| 15 | 45,X[?]/46,XX[?] | 1 | 1 | 1 | / | / | 未孕 |
| 16* | 45,X[5]/46,XX[45] | 1 | 1 | 1 | / | / | /# |
| 17* | 45,X[5]/46,XX[45] | 5 | 5 | 3 | / | -7(p22.1-pter);+17 | 未孕 |
| 18 | 45,X,15ps+[4]/46,XX,15ps+[114] | 4 | 4 | 1 | / | +19;-12(q24.31-qter);-16 | 活产 |
| 19 | 45,X[5]/46,XX[95] | 6 | 6 | 0 | +5(mos, 26%), -19(mos, 21%); -3(q11.2-qter)(mos, 32%), -16(mos, 26%), -18(p11.21-pter)(mos, 41%), +4(q13.1-qter)(mos, 25%), +7(q31.33-qter)(mos, 37%), +11(q14.3-qter)(mos, 34%), +13(q31.3-qter)(mos, 36%), +14(q22.3-qter)(mos, 51%); -1(mos, 23%), -16(mos,26%) | +21,-X(q25-qter)(mos, 42%); Triploid; Triploid | 自然流产 |
| 20 | 45,X[35]/46,X,del(p21) | 1 | 1 | 0 | -2(q14.1-qter)(mos, 29%) | / | 自然流产 |
| 21 | 45,X[49]/47,XXX[51] | 6 | 6 | 4 | +15(mos, 26%), +22(mos, 25%) | -18 | / |
| 小计 | 32 | 31 | 13 | 7 | 11 | ||
| 22 | 46,X,der(X)t(X;Y)(p22.3;q11.2) | 3 | 3 | 2 | / | -X(p22.31-pter), +Y(q11.221-qter) | / |
| 23 | 46,X,del(X)(p21) | 2 | 2 | 0 | +3(mos, 26%) | -X(p21.3-pter) | 活产 |
| 24 | 46,X,del(X)(q22.3q27.1) | 1 | 1 | 0 | / | -X(q22.3-q27.1) | / |
| 小计 | 6 | 6 | 2 | 1 | 3 | ||
| 总计 | 77 | 76 | 40 | 13 | 23 |
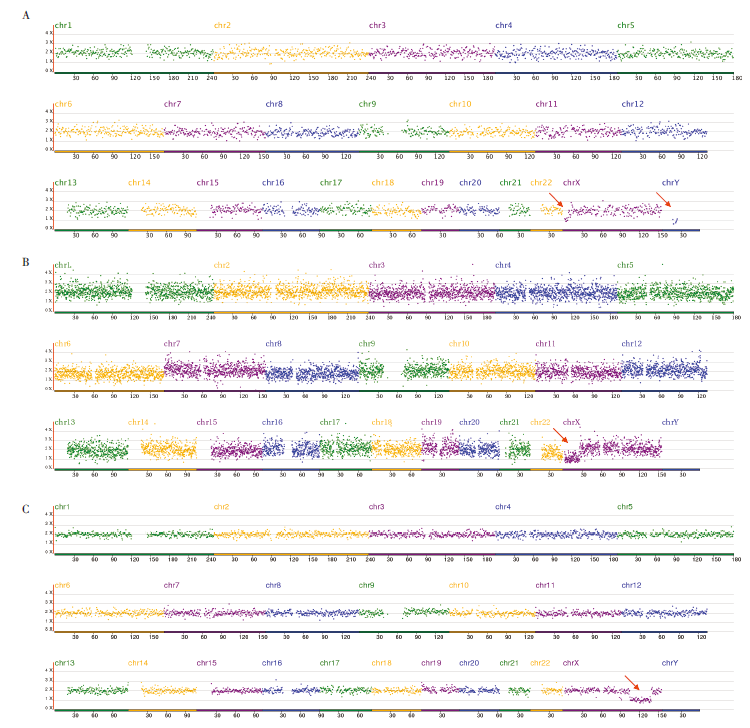
图1 X染色体节段性缺失女性PGT异常胚胎结果图注:图A示病例22异常胚胎遗传了母源的衍生染色体der(X)t(X;Y)(p22.3;q11.2);图B示病例23异常胚胎遗传了母源del(X)(p21);图C示病例24异常胚胎遗传了母源的del(X)(q22.3q27.1)。图中箭头所示为X染色体节段性缺失(病例22、23、24)及Y染色体片段信号(病例22)。
| [1] |
《胚胎植入前遗传学诊断/筛查专家共识》编写组. 胚胎植入前遗传学诊断/筛查技术专家共识[J]. 中华医学遗传学杂志, 2018, 35(2):151-155. doi: 10.3760/cma.j.issn.1003-9406.2018.02.001.
doi: 10.3760/cma.j.issn.1003-9406.2018.02.001 |
| [2] |
Demily C, Poisson A, Peyroux E, et al. Autism spectrum disorder associated with 49,XYYYY: case report and review of the literature[J]. BMC Med Genet, 2017, 18(1):9. doi: 10.1186/s12881-017-0371-1.
doi: 10.1186/s12881-017-0371-1 pmid: 28137251 |
| [3] |
《男性生殖遗传学检查专家共识》编写组, 中华医学会男科学分会. 男性生殖遗传学检查专家共识[J]. 中华男科学杂志, 2015, 21(12):1138-1142. doi: 10.13263/j.cnki.nja.2015.12.017.
doi: 10.13263/j.cnki.nja.2015.12.017 |
| [4] |
Fiorentino F, Biricik A, Bono S, et al. Development and validation of a next-generation sequencing-based protocol for 24-chromosome aneuploidy screening of embryos[J]. Fertil Steril, 2014, 101(5):1375-1382. doi: 10.1016/j.fertnstert.2014.01.051.
doi: 10.1016/j.fertnstert.2014.01.051 pmid: 24613537 |
| [5] |
Handyside AH, Kontogianni EH, Hardy K, et al. Pregnancies from biopsied human preimplantation embryos sexed by Y-specific DNA amplification[J]. Nature, 1990, 344(6268):768-770. doi: 10.1038/344768a0.
doi: 10.1038/344768a0 URL |
| [6] |
Zegers-Hochschild F, Adamson GD, Dyer S, et al. The International Glossary on Infertility and Fertility Care, 2017[J]. Fertil Steril, 2017, 108(3):393-406. doi: 10.1016/j.fertnstert.2017.06.005.
doi: S0015-0282(17)30429-6 pmid: 28760517 |
| [7] |
Gleicher N, Albertini DF, Patrizio P, et al. The uncertain science of preimplantation and prenatal genetic testing[J]. Nat Med, 2022, 28(3):442-444. doi: 10.1038/s41591-022-01712-7.
doi: 10.1038/s41591-022-01712-7 pmid: 35314820 |
| [8] |
Mastenbroek S, de Wert G, Adashi EY. The Imperative of Responsible Innovation in Reproductive Medicine[J]. N Engl J Med, 2021, 385(22):2096-2100. doi: 10.1056/NEJMsb2101718.
doi: 10.1056/NEJMsb2101718 URL |
| [9] |
沈鉴东, 吴畏, 高超, 等. 单细胞微阵列比较基因组杂交技术在胚胎植入前遗传学筛查中的应用[J]. 生殖医学杂志, 2012, 21(5):417-422. doi: 10.3969/j.issn.1004-3845.2012.05.001.
doi: 10.3969/j.issn.1004-3845.2012.05.001 |
| [10] | 沈鉴东, 吴畏, 蔡令波, 等. 微阵列比较基因组杂交技术在染色体易位胚胎植入前遗传学诊断中的应用[J]. 国际生殖健康/计划生育杂志, 2014, 33(3):165-167. |
| [11] |
沈鉴东, 吴畏, 舒黎, 等. 基于微阵列比较基因组杂交技术的胚胎植入前遗传学诊断和筛查在不同阶段胚胎中的临床应用结局分析[J]. 中华妇产科杂志, 2017, 52(12):828-834. doi: 10.3760/cma.j.issn.0529-567x.2017.12.007.
doi: 10.3760/cma.j.issn.0529-567x.2017.12.007 |
| [12] |
Jo WH, Jung MK, Kim KE, et al. XYY syndrome: a 13-year-old boy with tall stature[J]. Ann Pediatr Endocrinol Metab, 2015, 20(3):170-173. doi: 10.6065/apem.2015.20.3.170.
doi: 10.6065/apem.2015.20.3.170 pmid: 26512355 |
| [13] |
Gonzalez-Merino E, Hans C, Abramowicz M, et al. Aneuploidy study in sperm and preimplantation embryos from nonmosaic 47,XYY men[J]. Fertil Steril, 2007, 88(3):600-606. doi: 10.1016/j.fertnstert.2006.12.020.
doi: 10.1016/j.fertnstert.2006.12.020 pmid: 17517402 |
| [14] |
Shi Q, Martin RH. Multicolor fluorescence in situ hybridization analysis of meiotic chromosome segregation in a 47,XYY male and a review of the literature[J]. Am J Med Genet, 2000, 93(1):40-46. doi: 10.1002/1096-8628(20000703)93:1<40::aid-ajmg7>3.0.co;2-k.
doi: 10.1002/1096-8628(20000703)93:1<40::aid-ajmg7>3.0.co;2-k URL |
| [15] |
Blanco J, Egozcue J, Vidal F. Meiotic behaviour of the sex chromosomes in three patients with sex chromosome anomalies (47,XXY, mosaic 46,XY/47,XXY and 47,XYY) assessed by fluorescence in-situ hybridization[J]. Hum Reprod, 2001, 16(5):887-892. doi: 10.1093/humrep/16.5.887.
doi: 10.1093/humrep/16.5.887 pmid: 11331634 |
| [16] |
Tartaglia NR, Howell S, Sutherland A, et al. A review of trisomy X (47,XXX)[J]. Orphanet J Rare Dis, 2010, 5:8. doi: 10.1186/1750-1172-5-8.
doi: 10.1186/1750-1172-5-8 pmid: 20459843 |
| [17] |
Otter M, Schrander-Stumpel CT, Curfs LM. Triple X syndrome: a review of the literature[J]. Eur J Hum Genet, 2010, 18(3):265-271. doi: 10.1038/ejhg.2009.109.
doi: 10.1038/ejhg.2009.109 pmid: 19568271 |
| [18] |
Linden MG, Bender BG, Robinson A. Sex chromosome tetrasomy and pentasomy[J]. Pediatrics, 1995, 96(4 Pt 1):672-682.
pmid: 7567329 |
| [19] |
Ratcliffe S. Long-term outcome in children of sex chromosome abnormalities[J]. Arch Dis Child, 1999, 80(2):192-195. doi: 10.1136/adc.80.2.192.
doi: 10.1136/adc.80.2.192 pmid: 10325742 |
| [20] |
Masterson TA 3rd, Nassau DE, Ramasamy R. A clinical algorithm for management of fertility in adolescents with the Klinefelter syndrome[J]. Curr Opin Urol, 2020, 30(3):324-327. doi: 10.1097/MOU.0000000000000757.
doi: 10.1097/MOU.0000000000000757 pmid: 32235276 |
| [21] |
Staessen C, Tournaye H, Van Assche E, et al. PGD in 47,XXY Klinefelter′s syndrome patients[J]. Hum Reprod Update, 2003, 9(4):319-330. doi: 10.1093/humupd/dmg029.
doi: 10.1093/humupd/dmg029 pmid: 12926526 |
| [22] |
Friedler S, Raziel A, Strassburger D, et al. Outcome of ICSI using fresh and cryopreserved-thawed testicular spermatozoa in patients with non-mosaic Klinefelter′s syndrome[J]. Hum Reprod, 2001, 16(12):2616-2620. doi: 10.1093/humrep/16.12.2616.
doi: 10.1093/humrep/16.12.2616 pmid: 11726584 |
| [23] |
Berglund A, Viuff MH, Skakkebæk A, et al. Changes in the cohort composition of turner syndrome and severe non-diagnosis of Klinefelter, 47,XXX and 47,XYY syndrome: a nationwide cohort study[J]. Orphanet J Rare Dis, 2019, 14(1):16. doi: 10.1186/s13023-018-0976-2.
doi: 10.1186/s13023-018-0976-2 pmid: 30642344 |
| [24] |
Mortensen KH, Andersen NH, Gravholt CH. Cardiovascular phenotype in Turner syndrome--integrating cardiology, genetics, and endocrinology[J]. Endocr Rev, 2012, 33(5):677-714. doi: 10.1210/er.2011-1059.
doi: 10.1210/er.2011-1059 pmid: 22707402 |
| [25] |
Sun L, Wang Y, Zhou T, et al. Glucose Metabolism in Turner Syndrome[J]. Front Endocrinol(Lausanne), 2019, 10:49. doi: 10.3389/fendo.2019.00049.
doi: 10.3389/fendo.2019.00049 |
| [26] |
Calanchini M, Moolla A, Tomlinson JW, et al. Liver biochemical abnormalities in Turner syndrome: A comprehensive characterization of an adult population[J]. Clin Endocrinol(Oxf), 2018, 89(5):667-676. doi: 10.1111/cen.13811.
doi: 10.1111/cen.13811 URL |
| [27] |
Wegiel M, Antosz A, Gieburowska J, et al. Autoimmunity Predisposition in Girls With Turner Syndrome[J]. Front Endocrinol(Lausanne), 2019, 10:511. doi: 10.3389/fendo.2019.00511.
doi: 10.3389/fendo.2019.00511 |
| [28] |
Bernard V, Donadille B, Zenaty D, et al. Spontaneous fertility and pregnancy outcomes amongst 480 women with Turner syndrome[J]. Hum Reprod, 2016, 31(4):782-788. doi: 10.1093/humrep/dew012.
doi: 10.1093/humrep/dew012 URL |
| [29] |
Calanchini M, Aye C, Orchard E, et al. Fertility issues and pregnancy outcomes in Turner syndrome[J]. Fertil Steril, 2020, 114(1):144-154. doi: 10.1016/j.fertnstert.2020.03.002.
doi: S0015-0282(20)30246-6 pmid: 32622407 |
| [30] |
Doğer E, Çakıroğlu Y, Ceylan Y, et al. Reproductive and obstetric outcomes in mosaic Turner’s Syndrome: a cross-sectional study and review of the literature[J]. Reprod Biol Endocrinol, 2015, 13:59. doi: 10.1186/s12958-015-0055-7.
doi: 10.1186/s12958-015-0055-7 URL |
| [31] |
O′Donnell RL, Warner P, Lee RJ, et al. Physiological sex steroid replacement in premature ovarian failure: randomized crossover trial of effect on uterine volume, endometrial thickness and blood flow, compared with a standard regimen[J]. Hum Reprod, 2012, 27(4):1130-1138. doi: 10.1093/humrep/des004.
doi: 10.1093/humrep/des004 URL |
| [32] |
Abir R, Fisch B, Nahum R, et al. Turner′s syndrome and fertility: current status and possible putative prospects[J]. Hum Reprod Update, 2001, 7(6):603-610. doi: 10.1093/humupd/7.6.603.
doi: 10.1093/humupd/7.6.603 pmid: 11727869 |
| [1] | 杨琴, 王涵婷, 曹媛媛, 周军, 王桂玲. 白藜芦醇对卵巢颗粒细胞功能的调节[J]. 国际生殖健康/计划生育杂志, 2024, 43(6): 524-528. |
| [2] | 江楠, 赵晓丽, 栾祖乾, 黄志云, 夏天. 高龄女性卵母细胞内氧化应激与非整倍体相关性研究进展[J]. 国际生殖健康/计划生育杂志, 2024, 43(5): 415-419. |
| [3] | 李轩昂, 王婷婷, 相珊, 赵帅, 连方. 铁死亡在多囊卵巢综合征中的研究进展[J]. 国际生殖健康/计划生育杂志, 2024, 43(5): 425-429. |
| [4] | 张爱玉, 栾翠玉, 王冬梅, 蒋帅. IVF-ET不孕症患者就医延迟现状及影响因素分析[J]. 国际生殖健康/计划生育杂志, 2024, 43(3): 190-194. |
| [5] | 贺晴雯, 李喜红. 辅助生殖技术助孕患者的睡眠障碍及非药物干预的研究进展[J]. 国际生殖健康/计划生育杂志, 2024, 43(3): 234-237. |
| [6] | 高朝阳, 章宁晴, 陈琼华, 吴荣锋. 环状RNA在子宫内膜异位症不孕患者卵泡颗粒细胞中的作用[J]. 国际生殖健康/计划生育杂志, 2024, 43(3): 243-248. |
| [7] | 叶霖, 侯志金, 孟昱时. 西罗莫司在生殖领域的研究进展[J]. 国际生殖健康/计划生育杂志, 2024, 43(2): 132-137. |
| [8] | 郝佳丽, 何玉洁. 不孕不育人群生育生活质量评价及其影响因素分析[J]. 国际生殖健康/计划生育杂志, 2024, 43(2): 159-165. |
| [9] | 田文艳, 罗营, 李小燕, 颜琪, 薛凤霞, 王颖梅, 张慧英. 45,X/47,XYY性发育异常一例并文献复习[J]. 国际生殖健康/计划生育杂志, 2024, 43(1): 11-16. |
| [10] | 闻星星, 柴梦晗, 杨倪, 邹慧娟, 章志国, 李琳, 陈蓓丽. TUBB8基因c.154-156del杂合变异致卵母细胞成熟阻滞一例[J]. 国际生殖健康/计划生育杂志, 2024, 43(1): 17-19. |
| [11] | 张晓翠, 于丽菲, 杨跃伟, 刘云静, 黄卫东, 伊江燕, 张雪萍. 45,X/46,XY染色体嵌合型不育症一例[J]. 国际生殖健康/计划生育杂志, 2024, 43(1): 20-23. |
| [12] | 罗丽燕, 金叶, 史莉, 韩梅, 于然, 宋东红. 多囊卵巢综合征合并不孕患者病耻感现状及影响因素研究[J]. 国际生殖健康/计划生育杂志, 2024, 43(1): 6-10. |
| [13] | 王洁, 马翔. 尿酸与女性生殖系统疾病及妊娠结局的相关性[J]. 国际生殖健康/计划生育杂志, 2024, 43(1): 63-67. |
| [14] | 崔领兵, 田文艳. 第二性征正常的SRY阴性46,XX男性综合征一例并文献复习[J]. 国际生殖健康/计划生育杂志, 2023, 42(6): 454-456. |
| [15] | 沈凌超, 王鑫, 纪冬梅. 线粒体DNA 8344A>G突变导致线粒体遗传病的研究进展和防治策略[J]. 国际生殖健康/计划生育杂志, 2023, 42(6): 471-475. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||